Model Introduction
The Chronic Obstructive Pulmonary Disease (COPD) animal model is an experimental system that simulates core pathological features such as airflow limitation, chronic inflammation, and emphysema seen in human COPD. Based on key risk factors for COPD, the model is induced by single factors (e.g., cigarette smoke, proteases, harmful gases) or multi-factor combinations (e.g., cigarette smoke combined with lipopolysaccharide) to produce pathological changes similar to human COPD, providing a tool for revealing pathogenesis and evaluating treatment strategies.
Research Applications
This model is widely applied in the following research fields:
- Mechanism Exploration: Studying pathological mechanisms such as chronic airway inflammation, lung tissue remodeling, and protease imbalance.
- Drug Screening and Evaluation: Assessing the preclinical efficacy of new therapeutic strategies and medications.
- Acute Exacerbation Research: Simulating the process of acute exacerbation of COPD (AECOPD) by inoculating bacteria or viruses.
- Comorbidity Research: Constructing composite models to study systemic lesions associated with COPD (e.g., osteoporosis, cardiovascular disease).
- Traditional Chinese Medicine (TCM) Research: Constructing “syndrome-disease combination” models to conduct modern research on TCM syndromes (e.g., Lung-Spleen Qi Deficiency syndrome).
Experimental Design Key Points
- Experimental Animals: Rats and mice are commonly used; guinea pigs, pigs, etc., may also be selected based on requirements.
- Modeling Methods and Parameters:
- Cigarette Smoke Exposure: Animals are placed in a smoke chamber for long-term passive inhalation of smoke, typically lasting from several weeks to several months.
- Protease Induction: Direct degradation of lung elastic fibers through intratracheal administration of pancreatic elastase.
- Harmful Gas/Particulate Matter Exposure: Long-term exposure to sulfur dioxide, ozone, or fine particulate matter (PM).
- Multi-factor Combination: For example, superimposing intratracheal lipopolysaccharide (LPS) stimulation on the basis of cigarette smoke exposure.
- Acute Exacerbation Induction: Inoculating Streptococcus pneumoniae, Haemophilus influenzae, or influenza virus onto a stable model.
- Syndrome-Disease Combination Factors: Superimposing TCM modeling factors such as overstrain or irregular diet on the disease model.
- Administration Routes: Primarily include passive inhalation (smoke/gas) and airway administration (protease/LPS/pathogens).
Key Monitoring Indicators
- Pulmonary Function Testing: Assessing the presence of persistent airflow limitation; core indicators include Forced Vital Capacity (FVC), Forced Expiratory Volume in 0.3 seconds (FEV0.3), and the FEV0.3/FVC ratio.
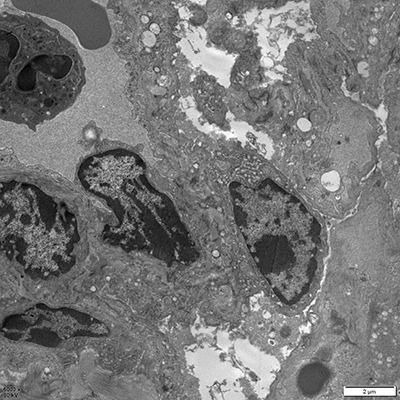
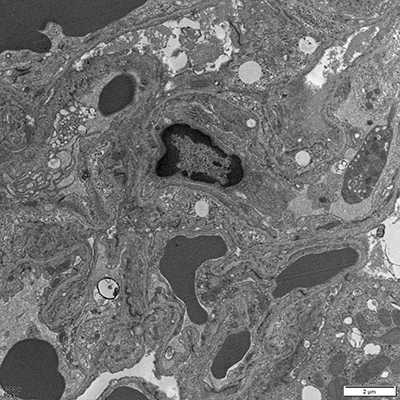
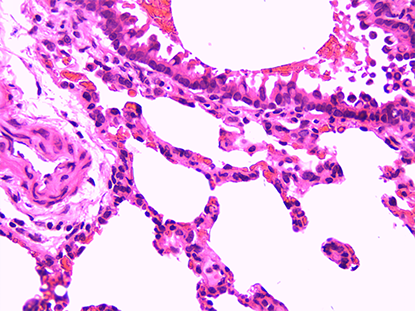
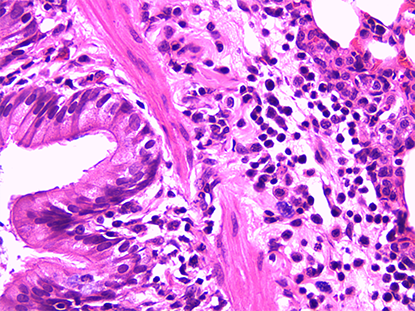
- Pathomorphological Examination: Utilizing H&E staining, Masson’s staining, etc., to observe airway inflammation, mucus hyperplasia, and alveolar structural destruction.
- Inflammatory and Biochemical Indicators:
- Cytological Classification: Detecting inflammatory cells in Bronchoalveolar Lavage Fluid (BALF).
- Cytokines: Detecting IL-8, TNF-α, etc., in BALF and lung tissue.
- Protease System: Evaluating the balance of protease systems such as MMP/TIMP.